
FOCUS QUESTION: How does stress make us more vulnerable to disease?
Not so long ago, the term psychosomatic described psychologically caused physical symptoms. In common usage, the term came to mean that the symptoms were unreal – ”merely” psychosomatic. To avoid such connotations and to better describe the genuine physiological effects of psychological states, most experts today refer instead to stress-related psycho-physiological illnesses, such as hypertension and some headaches. Stress also leaves us less able to fight off disease. The field of psychoneuroimmunology studies these mind-body interactions (Kiecolt-Glaser, 2009). This awkward name makes sense when said slowly: Your thoughts and feelings (psycho) influence your brain (neuro), which influences the endocrine hormones that affect your disease-fighting immune system. And this field is the study of (ology) those interactions.
Hundreds of experiments reveal the nervous and endocrine systems’ influence on the immune system (Sternberg, 2009).You can think of the immune system as a complex surveillance system. When it functions properly, it keeps you healthy by isolating and destroying bacteria, viruses, and other invaders. Four types of cells are active in these search-and-destroy missions (FIGURE 44.1). Two are types of white blood cells, called lymphocytes. B lymphocytes mature in the bone marrow and release antibodies that fight bacterial infections. T lymphocytes form in the thymus and other lymphatic tissue and attack cancer cells, viruses, and foreign substances – even “ good” ones, such as transplanted organs. The third agent is the macrophage (“big eater”), which identifies, pursues, and ingests harmful invaders and worn-out cells. And, finally, the natural killer cells (NK cells) pursue diseased cells (such as those infected by viruses or cancer). Your age, nutrition, genetics, body temperature, and stress all influence your immune system’s activity.
When your immune system doesn’t function properly, it can err in two directions. Responding too strongly, it may attack the body’s own tissues, causing some forms of arthritis or an allergic reaction. Underreacting, it may allow a dormant herpes virus to erupt or cancer cells to multiply. Women are immunologically stronger than men, making them less susceptible to infections, but this very strength also makes them more susceptible to self-attacking diseases, such as lupus and multiple sclerosis (Morell, 1995; Pido-Lopez et al., 2001).
Your immune system is not a headless horseman. The brain regulates the secretion of stress hormones, which suppresses the disease-fighting lymphocytes. Immune suppression appears when animals are stressed by physical restraints, unavoidable electric shocks, noise, crowding, cold water, social defeat, or separation from their mothers (Maier et al., 1994). One six-month study monitored immune responses in 43 monkeys (Cohen et al., 1992).
Twenty-one were stressed by being housed with new roommates – three or four new monkeys – each month. By the end of the experiment, the socially disrupted monkeys’ immune systems were weaker than those of monkeys left in stable groups. Human immune systems react similarly. Two examples:
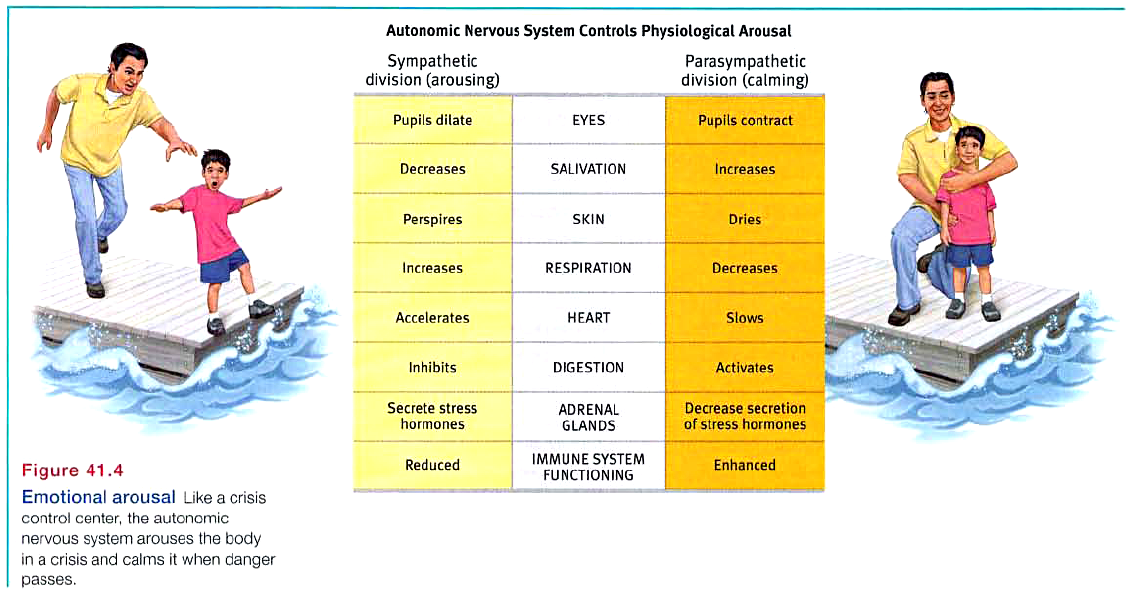
The stress effect on immunity makes physiological sense. It takes energy to track down invaders, produce swelling, and maintain fevers. Thus, when diseased, your body reduces muscular energy output by inactivity and increased sleep. Stress does the opposite. It creates a competing energy need. During an aroused fight-or-flight reaction, your stress responses divert energy from your disease-fighting immune system and send it to your muscles and brain (see Figure 41.4). This renders you more vulnerable to illness. The bottom line: Stress does not make us sick, but it does alter our immune functioning, which leaves us less able to resist infection.
Let’s consider some ways that stress might affect AIDS, cancer, and heart disease.
We know that stress suppresses immune functioning. What does this mean for people with AIDS (acquired immune deficiency syndrome)? As its name tells us, AIDS is an immune disorder, caused by the human immunodeficiency virus (HIV). AIDS has become the world’s fourth leading cause of death and Africa’s number one killer.
Ironically, if a disease is spread by human contact (as AIDS is, through the exchange of bodily fluids, primarily semen and blood), and if it kills slowly (as AIDS does), it can be lethal to more people. Those who acquire HIV often spread it in the highly contagious first few weeks before they know they are infected. Worldwide, some 2.6 million people – slightly more than half of them women – became infected with HIV in 2009, often without their awareness (UNAIDS, 2010). Years after the initial infection, when AIDS appears, people have difficulty fighting off other diseases, such as pneumonia. More than 25 million people worldwide have died of AIDS (UNAIDS, 2010). (In the United States, where “only” a half-million of these fatalities have occurred, AIDS has killed more people than did combat in all the twentieth-century wars.)
Stress cannot give people AIDS. But could stress and negative emotions speed the transition from HIV infection to AIDS in someone already infected? Might stress predict a faster decline in those with AIDS? The answer to both questions seems to be Yes (Bower et al., 1998; Kiecolt-Glaser & Glaser, 1995; Leserman et al., 1999). HIV-infected men who experience stressful events, such as the loss of a partner, exhibit somewhat greater immune suppression and travel a faster course in this disease.
Would efforts to reduce stress help control the disease? Again, the answer appears to be Yes. Educational initiatives, bereavement support groups, cognitive therapy, relaxation training, and exercise programs that reduce stress have all had positive consequences for HIV-positive people (Baum & Posluszny, 1999; McCain et al., 2008; Schneiderman, 1999). But the benefits are small, compared with available drug treatments.
Although AIDS is now more treatable than ever before, preventing HIV infection is a far better option. This is the focus of m.any educational programs, such as the ABC (abstinence, being faithful, condom use) program that has been used with seeming success in Uganda (Altm.an, 2004; USAID, 2004). In addition to such programs that seek to influence sexual norms and behaviors, today’s “combination prevention” programs also include medical strategies (such as drugs and male circumcision that reduce HIV transmission) and efforts to reduce social inequalities that increase HIV risk (UNAIDS, 2010).
Stress does not create cancer cells. But in a healthy, functioning immune system, lymphocytes, macro phages, and NK cells search out and destroy cancer cells and cancer-damaged cells. If stress weakens the immune system, might this weaken a person’s ability to fight off cancer? To explore a possible connection between stress and cancer, experimenters have implanted tumor cells in rodents or given them carcinogens (cancer-producing substances). They then exposed some rodents to uncontrollable stress, such as inescapable shocks, which weakened their immune systems. Those rodents were indeed more prone to developing cancer (Sklar & Anisman, 1981). Their tumors developed sooner and grew larger than in nonstressed rodents.
Does this stress-cancer link also hold with humans? The results are mixed. Some studies find that people are at increased risk for cancer within a year after experiencing depression, helplessness, or bereavement (Chida et al., 2008; Steptoe et al., 2010). In one large Swedish study, the risk of colon cancer was 5.5 times greater among people with a history of workplace stress than among those who reported no such problems. This difference was not attributable to group differences in age, smoking, drinking, or physical characteristics (Courtney et al., 1993). Other studies, however, have found no link between stress and human cancer (Coyne et al., 2010; Petticrew et al., 1999, 2002). Concentration camp survivors and former prisoners of war, for example, do not have elevated cancer rates.
One danger in hyping reports on emotions and cancer is that some patients may then blame themselves for their illness: “If only I had been more expressive, relaxed, and hopeful.” A corollary danger is a “wellness macho” among the healthy, who take credit for their “healthy character” and lay a guilt trip on the ill: “She has cancer? That’s what you get for holding your feelings in and being so nice.” Dying thus becomes the ultimate failure.
It’s important enough to repeat: Stress does not create cancer cells. At worst, it may affect their growth by weakening the body’s natural defenses against multiplying malignant cells (Antoni & Lutgendorf, 2007). Although a relaxed, hopeful state may enhance these defenses, we should be aware of the thin line that divides science from wishful thinking. The powerful biological processes at work in advanced cancer or AIDS are not likely to be cOlTlpletely derailed by avoiding stress or maintaining a relaxed but determined spirit (Anderson, 2002; Kessler et al., 1991). And that explains why research consistently indicates that psychotherapy does not extend cancer patients’ survival (Coyne et al., 2007, 2009; Coyne & Tennen, 2010).
FOCUS QUESTION: Why are some of us more prone than others to coronary heart disease?
Stress is much more closely linked to coronary heart disease, North America’s leading cause of death. In this disease, the blood vessels that nourish the heart muscle gradually close. Hypertension and a family history of the disease increase the risk of coronary heart disease. So do many behavioral factors (smoking, obesity, a high-fat diet, physical inactivity), physiological factors (an elevated cholesterol level), and psychological factors (stress responses and personality traits).
In some classic studies, Meyer Friedman, Ray Rosenman, and their colleagues tested the idea that stress increases vulnerability to heart disease by measuring the blood cholesterol level and clotting speed of 40 U.S. male tax accountants at different times of year (Friedman & Rosenman, 1974; Friedman & illmer, 1984). From January through March, the test results were completely normal. Then, as the accountants began scrambling to finish their clients’ tax returns before the April 15 filing deadline, their cholesterol and clotting measures rose to dangerous levels. In May and June, with the deadline past, the measures returned to normal. Stress predicted heart attack risk for these men. The researchers’ hunch had paid off, launching a classic nine-year study of more than 3000 healthy men, aged 35 to 59.
When organic causes of illness are unknown, it is tempting to invent psychological explanations. Before the germ that causes tuberculosis (TB) was discovered, personality explanations of TB were popular (Sontag, 1978).
In both India and America, Type A bus drivers are literally hard-driving: They brake, pass, and honk their horns more often than their more easygoing Type B colleagues (Evans et al., 1987).
At the start of the study, the researchers interviewed each man for 15 minutes, noting his work and eating habits, manner of talking, and other behavioral patterns. Those who seemed the most reactive, competitive, hard-driving, impatient, time-conscious, supermotivated, verbally aggressive, and easily angered they called Type A. The roughly equal number who were more easygoing they called Type B. Which group do you suppose turned out to be the most coronary-prone?
Nine years later, 257 men had suffered heart attacks, and 69 percent of them were Type A. Moreover, not one of the “pure” Type Bs – the most mellow and laid back of their group – had suffered a heart attack.
As often happens in science, this exciting discovery provoked enormous public interest. But after that initial honeymoon period, researchers wanted to know more. Was the finding reliable? If so, what is the toxic component of the Type A profile: Time-consciousness? Competitiveness? Anger?
More than 700 studies have now explored possible psychological correlates or predictors of cardiovascular health (Chida & Hamer, 2008; Chida & Steptoe, 2009). These reveal that Type Xs toxic core is negative emotions – especially the anger associated with an aggressively reactive temperament. As we will see in Module 83’s discussion of anger, when we are harassed or challenged, our active sympathetic nervous system redistributes bloodflow to our muscles, pulling it away from our internal organs. One of those organs, the liver, which normally removes cholesterol and fat from the blood, can’t do its job. Type A individuals are more often “combat ready.” Thus, excess cholesterol and fat may continue to circulate in their blood and later get deposited around the heart. Further stress – sometimes conflicts brought on by their own abrasiveness – may trigger altered heart rhythms. In people with weakened hearts, this altered pattern can cause sudden death (Kamarck & Jennings, 1991). Hostility also correlates with other risk factors, such as smoking, drinking, and obesity (Bunde & Suls, 2006). In important ways, people’s minds and hearts interact.
Hundreds of other studies of young and middle-aged men and women have confirmed the finding that people who react with anger over little things are the most coronary-prone. Suppressing negative emotions only heightens the risk (Kupper & Denollet, 2007). One study followed 13,000 middle-aged people for 5 years. Among those with normal blood pressure, people who had scored high on anger were three times more likely to have had heart attacks, even after researchers controlled for smoking and weight (Williams et al., 2000). Another study followed 1055 male medical students over an average of 36 years. Those who had reported being hot tempered were five times more likely to have had a heart attack by age 55 (Chang et al., 2002). As others have noted, rage “seems to lash back and strike us in the heart muscle” (Spielberger & London, 1982).
Pessimism seems to be similarly toxic. One study followed 1306 initially healthy men who a decade earlier had scored as optimists, pessimists, or neither. Even after other risk factors such as smoking had been ruled out, pessimists were more than twice as likely as optimists to develop heart disease (FIGURE 44.3) (Kubzansky et al., 2001).
Depression, too, can be lethal. Happy people tend to be healthier and to outlive their unhappy peers (Diener & Chan, 2011; Siahpush et al., 2008). Even a big, happy smile predicts longevity, as Ernest Abel and Michael Kruger (2010) discovered when they examined the photographs of 150 Major League Baseball players who had appeared in the 1952 Baseball Register and had died by 2009. On average, the non-smilers had died at 73, compared with an average 80 years for those with a broad, genuine smile.
The accumulated evidence from 57 studies suggests that “depression substantially increases the risk of death, especially death by unnatural causes and cardiovascular disease” (Wulsin et al., 1999). After following 63,469 women over a dozen years, researchers found more than a doubled rate of heart attack death among those who initially scored as depressed (Whang et al., 2009). In the years following a heart attack, people with high scores for depression are four times more likely
than their low-scoring counterparts to develop further heart problems (Frasure-Smith & Lesperance, 2005). Depression is disheartening. Depressed people tend to smoke more and exercise less (Whooley et al., 2008), but stress itself is also disheartening:
Research suggests that heart disease and depression may both result when chronic stress triggers persistent inflammation (Matthews, 2005; Miller & Blackwell, 2006). After a heart attack, stress and anxiety increase the risk of death or of another attack (Roest et al., 2010). As we have seen, stress disrupts the body’s disease-fighting immune system, enabling the body to focus its energies on fleeing or fighting the threat. Yet stress hormones enhance one immune response, the production of proteins that contribute to inflammation. Thus, people who experience social threats, including children raised in harsh families, are more prone to inflammation responses (Dickerson et al., 2009; Miller & Chen, 2010). Inflammation fights infections; if you cut yourself, inflammation recruits infection-fighting cells. But persistent inflammation can produce problems such as asthma or clogged arteries, and worsen depression (see FIGURE 44.4). Researchers are now uncovering the molecular mechanisms by which stress, in some people, activates genes that control inflammation (Cole et al., 2010).
Behavioral medicine research provides a reminder of one of contemporary psychology’S overriding themes: Mind and body interact; everything psychological is simultaneously physiological. Psychological states are physiological events that influence other parts of our physiological system. Just pausing to think about biting into an orange section – the sweet, tangy juice from the pulpy fruit flooding across your tongue – can trigger salivation. As the Indian sage Santi Parva recognized more than 4000 years ago, “Mental disorders arise from physical causes, and likewise physical disorders arise from mental causes.” There is an interplay between our heads and our health. We are biopsychosocial systems.
Stress and Susceptibility to Disease
Stress and AIDS
Stress and Cancer
Stress and Heart Disease
Before You Move On
ASK YOURSELF: Are there changes you could make to avoid the persistent stressors in your life?
TEST YOURSELF: Which component of the Type A personality has been linked most closely to coronary heart disease?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}